Ethylenediaminetetraacetic acid — EDTA — is not a drug in the traditional sense. It is a precisely structured ligand: a molecule engineered by chemistry to grip heavy metal ions with the mechanical certainty of a claw.
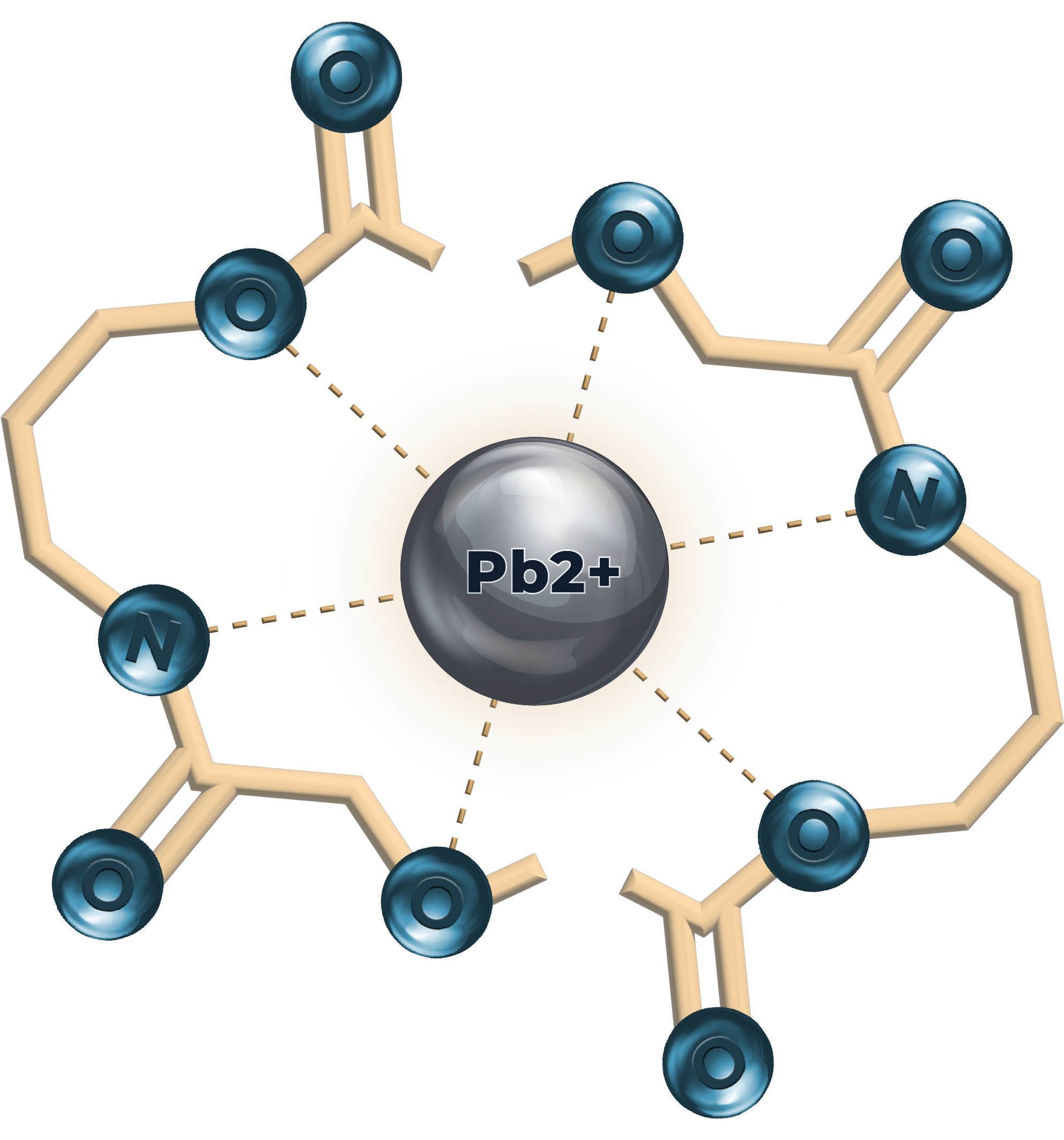
EDTA belongs to a class of compounds called polyaminocarboxylic acids. Its structure features two central nitrogen atoms and four carboxylate (–COO-) groups — six electron-donating sites in total. In solution, these six "arms" fold simultaneously around a positively charged metal ion, forming what chemists call an octahedral coordination complex.
The resulting bond is not a simple ionic attraction. It is a chelate ring — from the Greek chēlē, meaning claw — in which the metal ion becomes caged within the molecular architecture. The stability of this cage is measured by the formation constant (Kf), which for EDTA–lead approaches 1018, meaning the bond is essentially irreversible under physiological conditions.
Once EDTA wraps around a lead or cadmium ion, that metal is effectively neutralized — stripped of its ability to interfere with enzymatic reactions, bind to DNA, or generate reactive oxygen species. The chelate complex is then excreted intact through the kidneys.
EDTA does not bind all metals equally. Its affinity follows a known selectivity sequence: lead and cadmium are bound significantly more tightly than calcium or magnesium. This differential affinity is the biochemical rationale for clinical chelation — under appropriate conditions, toxic heavy metals are preferentially sequestered.
However, this selectivity is concentration-dependent. At very high doses, EDTA will also bind essential minerals, which is the basis for the critical mineral replenishment protocol discussed in Section 04.
EDTA molecules enter the bloodstream or interstitial fluid, where they encounter free and loosely-bound heavy metal ions displaced from cellular binding sites.
The six donor atoms of EDTA orient simultaneously around the target metal ion. Each donor atom donates an electron pair to the metal's vacant d-orbital, forming up to six coordinate bonds.
The resulting chelate ring structure achieves thermodynamic stability (log Kf ≈ 18.0 for Pb²+). The metal is no longer biologically reactive — it cannot participate in redox cycling or enzyme inhibition.
The EDTA–metal complex is water-soluble and filtered at the glomerulus. The intact chelate is excreted in urine within 24–48 hours, permanently removing the metal from the body.
Lead's toxicity is, in large part, a case of molecular mistaken identity. Understanding this confusion is the key to understanding why chelation works — and why lead is so insidiously harmful.
The body's cellular machinery doesn't recognize atoms by name — it recognizes them by charge and size. Calcium (Ca²+) carries a +2 charge and an ionic radius of 1.00 Å. Lead (Pb²+) also carries a +2 charge and an ionic radius of 1.19 Å — close enough that the body's calcium transport proteins, channel gates, and receptor binding sites simply cannot tell them apart. When lead enters the bloodstream, the cell opens its door thinking it's receiving calcium. This is the mistaken identity: not a metaphor, but a literal failure of molecular recognition happening at the atomic scale, billions of times per second
Essential mineral. Admitted freely by calcium channels and transport proteins throughout the body. Behaves correctly once inside — triggering controlled signaling, muscle contraction, and enzyme regulation.
Toxic heavy metal. Gains cellular entry by passing as calcium. Once inside, it behaves nothing like calcium — hijacking signaling proteins, blocking enzyme reactions, and generating oxidative damage the cell has no defense against.
Calcium ions are the primary signaling currency of human physiology. They trigger muscle contraction through troponin, regulate synaptic transmission, and control dozens of enzyme cascades. Every cell maintains exquisite calcium homeostasis across its membrane — a gradient essential for life.
Lead ions exploit the same molecular machinery designed for calcium. Calcium transport proteins like calmodulin and protein kinase C bind lead even more tightly than calcium — up to 10,000 times more tightly in some cases. Once inside a cell, lead permanently disrupts signaling, inhibits heme synthesis, and generates oxidative stress that calcium never would.
Lead stored in bone is the central problem. Bone acts as a long-term reservoir, releasing lead slowly into the bloodstream over decades — especially during pregnancy, menopause, or aging when bone turnover accelerates. Sweat, dietary fiber, and antioxidant protocols cannot mobilize bone-sequestered lead in any meaningful quantity.
EDTA works differently. By aggressively chelating free lead ions in the bloodstream, it creates a concentration gradient — blood lead drops, and the body's own equilibrium chemistry draws stored lead out of bone back into circulation to restore balance. EDTA then catches it again. Each cycle pulls another layer of sequestered lead out of tissue. It is a gradual, chemistry-driven draw-down that works with the body's equilibrium dynamics, not against them.
Here is where the apparent paradox resolves. The body recognizes ions by charge and size — which is why it confuses lead for calcium. EDTA recognizes ions by electron configuration and binding affinity — an entirely different system. Lead's d-orbital electron structure makes it bind EDTA's six coordination sites far more tightly than calcium does.
The result: EDTA's formation constant for lead is 18.0; for calcium it is 10.7. That 7-point logarithmic difference means EDTA grabs lead approximately 10 million times more readily than calcium in a competitive environment. The body's mistake is EDTA's advantage — the same properties that make lead a convincing calcium impostor also make it a preferential EDTA target.
Because EDTA binds ionic calcium — calcium dissolved in biological fluids — researchers have proposed that this secondary effect may itself be therapeutically relevant in conditions where calcium accumulates in places it should not be.
Atherosclerotic plaques contain significant calcium deposits. Researchers have proposed that EDTA's ability to chelate ionic calcium from arterial walls may contribute to the cardiovascular signals observed in the original TACT trial — though the dedicated follow-up trial TACT2 (2024) did not reproduce TACT's cardiovascular event reduction. The mechanism remains an active area of investigation, with growing evidence that EDTA's heavy-metal-removing properties may play as significant a role as its direct calcium-binding effects.
Calcium can accumulate in soft tissues — muscles, tendons, and joints — in conditions associated with aging, chronic inflammation, and metabolic dysfunction. This ectopic calcification is distinct from normal bone mineralization. Some researchers propose that chelation therapy may help mobilize these misplaced calcium deposits, though controlled clinical evidence in this specific area remains limited.
One of the most common — and understandable — concerns raised about chelation therapy is whether removing calcium from the body weakens the bones. The science provides clear reassurance: EDTA cannot meaningfully chelate calcium that is structurally bound within the bone matrix.
Crystalline hydroxyapatite — solid mineral lattice tightly bound within the bone matrix. Structurally inaccessible to EDTA at therapeutic doses.
Free calcium ions dissolved in biological fluids — bloodstream, extracellular matrix, soft tissue deposits. These are the ions EDTA chelates and removes.
This is one of the most common and understandable concerns raised about chelation therapy, and the science provides clear reassurance. Bone mineral — the calcium that gives bone its structural strength — exists as crystalline hydroxyapatite (Ca₁₀(PO₄)₆(OH)₂), a solid mineral lattice tightly bound within the bone matrix. EDTA chelates ionic calcium: free Ca²⁺ ions dissolved in biological fluids.
These are fundamentally different states of calcium. EDTA cannot meaningfully dissolve or remove calcium from an intact crystalline bone matrix at therapeutic doses — the same way a magnet can pick up loose iron filings but cannot strip iron from a steel beam. At therapeutic doses, studies have not demonstrated clinically significant reductions in bone mineral density.
This remains an important area of monitoring in long-term chelation protocols, and maintaining adequate dietary and supplemental calcium intake — as described in Section 04 — provides an additional layer of protection.
EDTA's chemistry is only half the equation. Even the most precisely engineered chelating agent is only as effective as its ability to reach the bloodstream. This is where delivery science becomes biology.
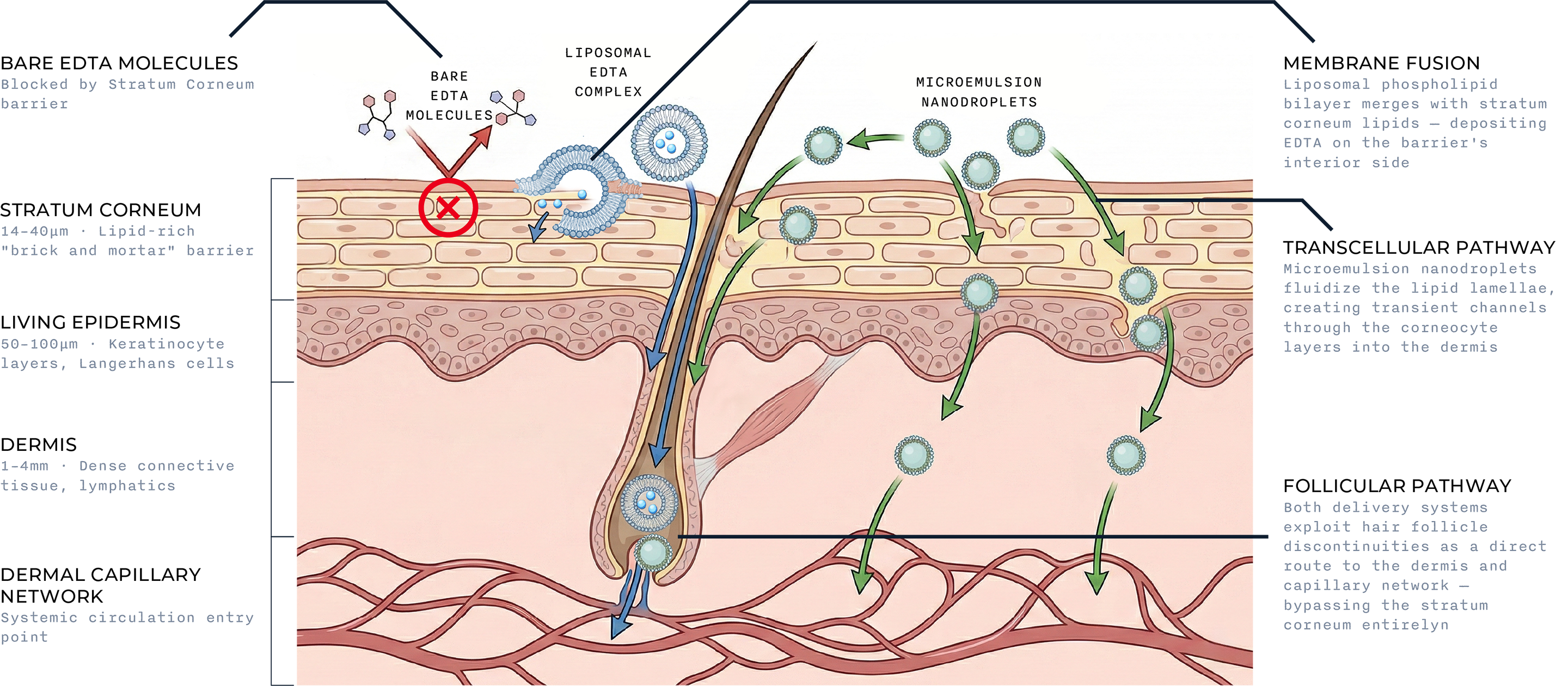
Two distinct phospholipid-based systems have been developed to solve the stratum corneum barrier — each working through a different mechanism, both reaching the same destination.
A phospholipid liposome — a nanoscale vesicle with a bilayer membrane structurally identical to a cell membrane — solves this problem not by forcing a water-soluble molecule through a lipid barrier, but by becoming part of the barrier itself.
When a liposome contacts the stratum corneum's lipid lamellae, its outer phospholipid shell undergoes membrane fusion: the two bilayers merge, depositing the liposome's aqueous payload — the EDTA — on the interior side of the barrier. From there, the molecule moves down its concentration gradient through the living epidermis and into the dermis, where the capillary network provides access to systemic circulation.
A second penetration route operates in parallel: follicular delivery. Hair follicles create discontinuities in the stratum corneum, providing direct channels into the dermis. Liposomes in the 100–200nm size range are well-suited to follicular penetration and represent a significant supplementary pathway.
Where liposomes work by becoming part of the barrier, a phospholipid microemulsion works by temporarily reorganizing it. A microemulsion is a thermodynamically stable system in which oil, water, and surfactants form nanoscale droplets that coexist in a single homogeneous phase — unlike an emulsion, it does not separate over time.
When applied to skin, the surfactant component fluidizes the lipid lamellae of the stratum corneum, creating transient channels through which polar molecules like EDTA can pass. Simultaneously, the high-phosphatidylcholine component provides genuine skin-membrane affinity — phospholipids naturally associate with the lipid environment of cell membranes, facilitating deeper penetration than a surfactant system alone.
The follicular pathway operates here as well. Microemulsion nanodroplets are well-sized to exploit hair follicle discontinuities as a direct route into the dermis, operating in parallel to the transcellular mechanism.
Both architectures share the same foundational logic: phospholipid affinity for the skin's lipid environment. The difference is mechanism — fusion versus disruption — not destination. In either case, formulation quality is the determining variable. The concentration and purity of phosphatidylcholine, vesicle size, droplet architecture, and pH all determine whether a delivery system actively reaches the dermis or remains at the skin surface.
Not all phospholipid delivery systems are equivalent. In liposomal formulations, vesicle size (100–200nm), membrane composition, encapsulation efficiency, and zeta potential all determine whether a liposome successfully fuses with skin or simply sits on the surface. In microemulsion systems, the ratio of phosphatidylcholine to surfactant, PC purity grade, droplet size, and pH determine whether the formulation actively penetrates the dermis or remains at the stratum corneum surface. The science of transdermal delivery lives in these formulation details — which is why evaluating a specific product's formulation matters as much as the delivery route itself. A full comparison of chelation delivery methods is available on The Comparison page →
Oral chelation works through a fundamentally different mechanism than IV or transdermal delivery. Most of EDTA's activity in oral form occurs not in the bloodstream — but in the digestive tract itself, before food and water are absorbed.
Oral EDTA has approximately 5% bioavailability — meaning only about 5% of an oral dose reaches systemic circulation in active form. For most pharmaceuticals, this would be a serious limitation. For oral EDTA's specific use case, it's by design.
The remaining 95% stays in the gastrointestinal tract, where it does the job it was given: binding heavy metals from food, water, and digestive secretions before those metals can be absorbed into the body.
Reaches systemic circulation
Stays in the gut — binding heavy metals from food, water, and bile before they're absorbed.
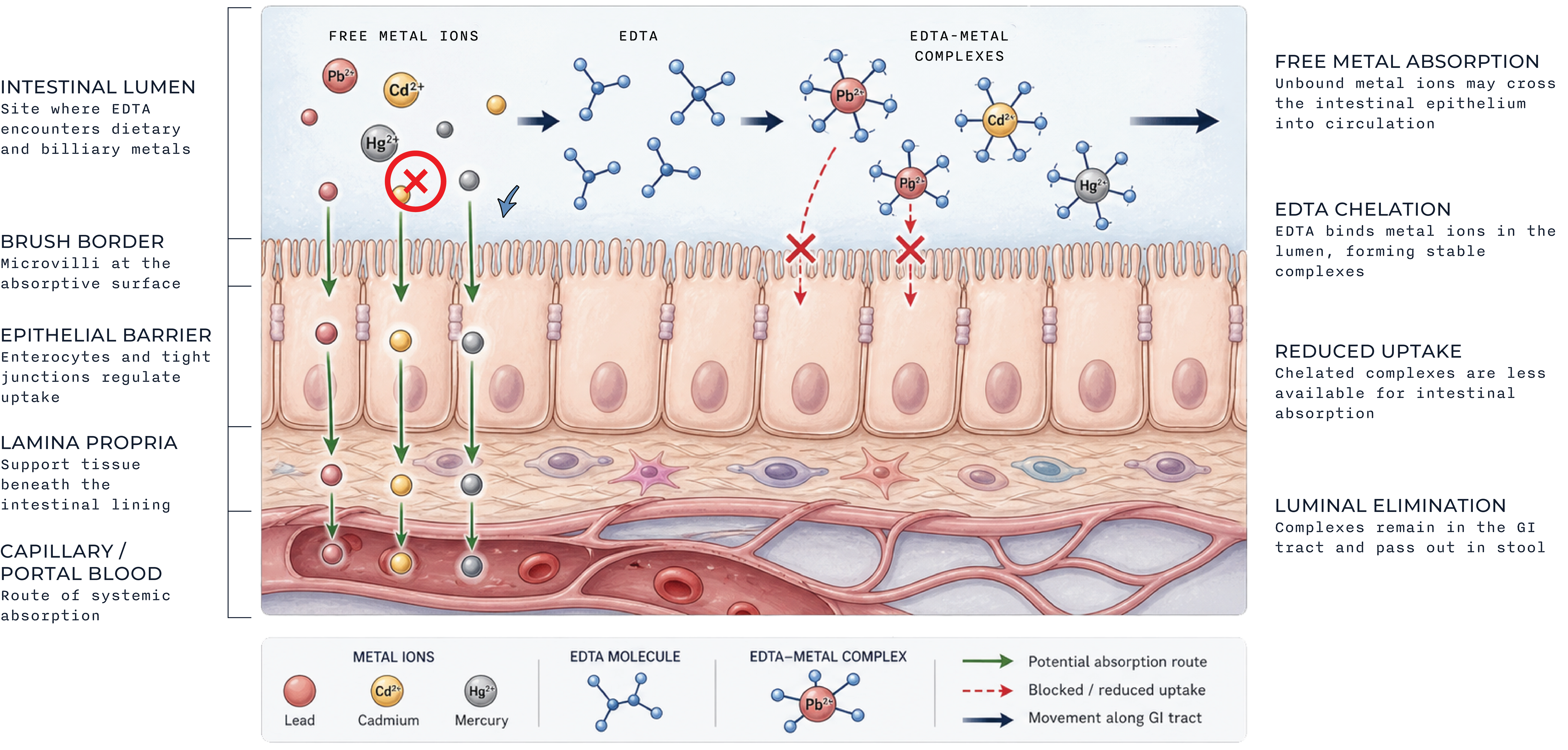
When EDTA enters the stomach and small intestine, it encounters lead, mercury, cadmium, and arsenic ions present in:
EDTA binds these metals into stable chelate complexes. Once bound, the metals lose their ability to be absorbed across the intestinal wall. Instead of entering the bloodstream, they pass through the digestive tract and are excreted in stool.
The three delivery methods serve different purposes:
Clears established systemic burden, used for confirmed acute toxicity
Gradual systemic turnover via skin and capillary network
Prevents new dietary and environmental absorption at the gut level
These are complementary mechanisms, not redundant ones. Oral EDTA's role is preventive and maintenance — reducing the ongoing exposure burden adults face daily — not a substitute for IV when systemic burden is confirmed.
Even though oral EDTA acts primarily in the GI tract, the small fraction that does reach systemic circulation — and the metals it binds within the gut — still affect mineral status over time. Long-term oral chelation protocols benefit from the same mineral replenishment principles described in the next section, though the magnitude of mineral disruption is generally smaller than with IV or transdermal protocols.
This is perhaps the most clinically important concept in chelation science — and the one most frequently omitted. EDTA does not discriminate between toxic heavy metals and essential trace minerals your body genuinely needs. Any responsible chelation protocol includes active mineral replenishment.
Required for over 300 enzymatic reactions. Critical for immune function, wound healing, protein synthesis, DNA transcription, and insulin regulation. One of the minerals most readily chelated alongside heavy metals.
Cofactor in over 600 enzyme systems including those governing energy production (ATP synthesis), DNA repair, and nerve conduction. Magnesium deficiency is already endemic in the developed world — chelation can compound this.
The most abundant mineral in the body, with 99% stored in bone and teeth. While EDTA's affinity for calcium is lower than for heavy metals, chronic chelation can incrementally affect serum calcium — making dietary and supplemental intake critical.
Essential for iron metabolism, connective tissue formation, and function of superoxide dismutase — the body's primary antioxidant enzyme. Copper is bound by EDTA with moderate affinity and should be monitored during extended chelation protocols.
Practitioners experienced with chelation therapy routinely recommend spacing mineral supplementation 2–4 hours away from EDTA administration — a timing window that allows chelation to occur without immediately binding the supplemented minerals. Comprehensive multimineral supplements, combined with a diet rich in mineral-dense whole foods, form the foundation of responsible long-term chelation practice. Consult a qualified healthcare practitioner before beginning any chelation protocol.
Precision in language is precision in science. These definitions are provided so that every claim on this site can be understood in its exact molecular context
A molecule or ion that donates a pair of electrons to a central metal atom or ion, forming a coordination complex. The word derives from the Latin ligare, "to bind." EDTA is a hexadentate ligand — it has six electron-donating sites.
In practice: EDTA acts as a ligand when it wraps its six arms around a lead ion, neutralizing its biological activity.
The fraction of an administered dose of a substance that reaches the systemic circulation in an unchanged, active form. An IV drug has 100% bioavailability by definition; oral drugs vary widely based on absorption and first-pass metabolism.
In practice: Oral EDTA has ~5% bioavailability. Delivery technology (such as liposomal encapsulation) aims to increase this figure by protecting the molecule during absorption.
An imbalance between the production of reactive oxygen species (free radicals) and the biological system's ability to neutralize them with antioxidants. Heavy metals catalyze free radical production through the Fenton and Haber-Weiss reactions.
In practice: Lead and cadmium generate oxidative stress that damages cell membranes, proteins, and DNA — contributing to cardiovascular disease, neurodegeneration, and cancer risk.
The formation of multiple coordinate bonds between a polydentate ligand and a single central metal atom. The term comes from the Greek chēlē (claw). Chelation produces a ring-like structure that dramatically increases the stability of the metal-ligand complex.
In practice: Chelation therapy applies this chemical principle therapeutically — using EDTA or similar ligands to sequester and remove heavy metals from biological tissue.
A transdermal delivery architecture using phosphatidylcholine to carry hydrophilic molecules through the stratum corneum. Two systems: liposomes, which penetrate via membrane fusion; and microemulsions, which penetrate by fluidizing the lipid barrier. Different mechanisms, same destination.
In practice: Plain EDTA cannot cross the stratum corneum unaided. A phospholipid delivery system bypasses the barrier entirely — formulation quality determines how effectively.
Also called the stability constant (Kf), this dimensionless number expresses the equilibrium constant for the formation of a complex in solution. A higher value indicates greater thermodynamic stability. Values are often expressed as logarithms (log Kf).
In practice: EDTA's log Kf for lead is 18.0, versus 10.7 for calcium. This 10-million-fold difference in binding affinity is why EDTA preferentially removes lead over calcium at therapeutic concentrations.
The phenomenon where the concentration of a drug is greatly reduced before it reaches systemic circulation, due to absorption by the gut wall and immediate metabolism by the liver following oral ingestion. This is the primary reason oral bioavailability is often dramatically lower than IV bioavailability.
In practice: Oral EDTA is subject to significant first-pass reduction. The transdermal route bypasses the liver entirely, delivering the molecule directly into the dermal capillary bed.
A calcium-binding messenger protein found in all eukaryotic cells. Calmodulin undergoes a conformational change when it binds calcium ions, activating numerous downstream enzyme systems. It is a central mediator of calcium's intracellular signaling role.
In practice: Lead ions bind calmodulin with far greater affinity than calcium — effectively hijacking the protein and triggering uncontrolled downstream signaling. This is a primary molecular mechanism of lead neurotoxicity.
A category of metallic elements with relatively high densities and atomic weights. In clinical toxicology, the term refers specifically to elements that are toxic to humans at low concentrations — including lead (Pb), mercury (Hg), cadmium (Cd), and arsenic (As). Unlike organic toxins, heavy metals cannot be metabolized and must be physically removed.
In practice: Because heavy metals accumulate in tissue over time and are not biodegradable by the body, chelation provides one of the only mechanisms for their physical elimination.
These perspectives are drawn from independent researchers and clinicians with no commercial association with this website. Their work forms the foundation of modern environmental medicine.
The literature has been showing for many years that lead causes hypertension, stroke, and cardiovascular disease. This study now shows that the cardiovascular toxicity of lead extends down to lower levels than were previously examined.
These metals interfere with essential biological functions and affect most populations on a global scale. After exposure, lead and cadmium accumulate in the body and remain in bones and organs for decades.
Previous estimates relied on the assumption that there is a threshold for the cardiovascular toxicity of lead. We found that there was no threshold. The hazard ratio or relative risk increased steeply at the lowest levels of exposure.